In a new study, researchers investigated the mortality and respiration rates of RNA virus-infected male fruit flies and how aging impacts these outcomes and measurements.
RNA viruses are responsible for approximately 70% of emerging infectious diseases in humans, according to a 2020 report by the National Academy of Medicine. Examples of RNA viruses include: influenza, hepatitis C, HIV, measles, zika, ebola, poliovirus, rhinovirus, rabies, and SARS-CoV-2—the virus responsible for the COVID-19 pandemic. After infection with an RNA virus, significant changes can take place in the host’s metabolism. While it is clear that disease tolerance declines as humans age, it is not yet clear how aging affects virus-induced changes in metabolism.
“Virus-induced metabolic reprogramming could impact infection outcomes, however, how this is affected by aging and impacts organismal survival remains poorly understood.”
An organism’s metabolism depends on oxygen to produce energy. An efficient immune system depends, in part, on energy from the body’s metabolism to fuel it. Paradoxically, decreased metabolism, or hypometabolism, is a survival strategy that promotes disease tolerance in response to infection. In this study, the researchers used oxygen consumption rate (OCR) to indirectly measure changes in metabolism before and after RNA viral infection. The team infected male fruit flies with the RNA virus Flock House virus (FHV), and documented their oxygen consumption rate and/or mortality times at different time intervals after infection.
“As the exact mechanisms by which hypometabolism promotes tolerance are not fully understood, D. melanogaster could serve as an excellent model to dissect the genetic and molecular bases of this process.”
After the first 72-hours post-infection, FHV appeared to modulate respiration in all flies, but age did not appear to have a significant effect on OCR. However, over the course of the three-day experiment, the longitudinal assessment showed that OCR in young flies progressively and significantly decreased, while OCR in aged flies remained constant. The researchers found that the OCR at 24-hours varied in response to both experimental treatment and survival status. FHV-injected flies that died prior to 48- or 72-hours had a lower OCR compared to survivors at 48-hours.
“Our results show that FHV infection significantly reduces organismal OCR compared to Tris-injected controls; however, we did not observe a significant change in OCR with aging. Interestingly, flies that died prior to 48-hours post-treatment measurements exhibited a significantly lower OCR at 24 h post-treatment compared to survivors. These findings suggest that the host’s metabolic profile could influence the outcome of viral infections.”
Conclusion
In conclusion, RNA viruses pose a significant threat to human health, causing numerous emerging infectious diseases. The impact of these viruses on the host’s metabolism, particularly in relation to aging, remains poorly understood. The recent study by Hagedorn et al. sheds light on the interaction between RNA viruses, metabolism and aging by examining the effects of the Flock House virus on the respiration rate of male fruit flies. The findings suggest that this infection can modulate the host’s OCR, and that the metabolic profile of the host could influence the outcome of viral infections. The authors suggest that further research is needed to determine the precise mechanisms by which RNA viruses affect metabolic rate and to explore the potential for interventions to modulate metabolic rate and improve healthspan and lifespan.
“Older flies exhibit impaired disease tolerance to FHV [19], and here we show that metabolic rate depression does not occur in older flies in response to FHV in the first three days following treatment. It is therefore possible that as is the case in mammals, flies employ hypometabolism as a survival strategy that is part of a disease tolerance mechanism. It would be interesting in the future to test this hypothesis by comparing OCR in tolerance mutant flies such as the G9a mutants.”
Click here to read the full research paper published by Aging.
Aging is an open-access, peer-reviewed journal that has been publishing high-impact papers in all fields of aging research since 2009. These papers are available to readers (at no cost and free of subscription barriers) in bi-monthly issues at Aging-US.com.
Click here to subscribe to Aging publication updates.
Behind the Study is a series of transcribed videos from researchers elaborating on their recent oncology-focused studies published by Aging. Visit the AgingYouTube channel for more insights from outstanding authors.
—
It’s David Sinclair here. I’m talking to you from my home in Boston during this pandemic stayed home time, but also wanted to talk to you about a new paper that we have coming out, or just came out in our journal, Aging, and its title is, “Why Does COVID-19 Disproportionately Affect the Elderly?”—which has become one of the biggest questions I think in this whole pandemic. And, if we could understand why the elderly were more susceptible, first of all, we could help them survive and have less severe cases, but also we could learn perhaps why younger people are also more susceptible. One thing that I often hear when I pose that question is oh, it’s just that old people are sicker and they die. Well, that’s not a good enough explanation because the elderly, even if they are healthy, have a much greater chance of dying than someone whose say, less than 65.
In fact, of all the main causes of death or risk factors in COVID-19, age is by far the most important one, independent of all those other risk factors. So a study just came out in the UK that looked at 17 million people that had COVID-19 and they could tell us based on that, what the ranking of the what’s called the hazard ratio of which symptoms and which lifestyle and cobalt morbidities track with COVID-19 more fatality risk.
And actually, in order starting with number five, it was diabetes/obesity. Number three was being male, that’s fairly risky. Having cancer of the blood was bad, which makes sense because you’ve disrupted your immune system. But by far the riskiest thing is age, independent of all these other things. In fact, compared to these other risks, age is basically the major determinate. If you’re 80, numbers where you’re about tenfold higher to someone who’s in their late 50s. So that led us to try to figure out what is going on with the age that makes them more susceptible. And again, it’s not just that those people start out sicker. And so we’ve written this perspective and gathered a lot of data from around the world, papers that have come out, papers that have been in publication. So in this perspective, we’ve gathered a lot of data from around the world, new papers, old papers, and really put together a list of things that we think are the most likely explanations for the elderly succumbing to COVID-19, independent of their actual underlying diseases and frailty.
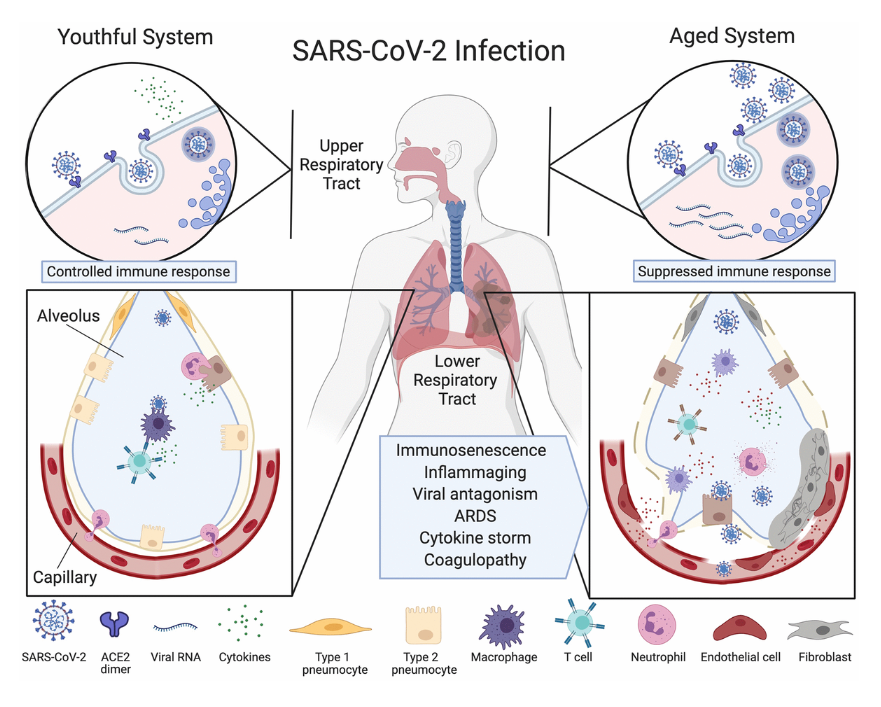
Figure 1. Ineffective clearance of SARS-CoV-2 infection in the aged respiratory system.
So let’s first go through one of the figures—you’ll see figure one is a beautiful illustration drawn by my wonderful coauthors, Amber Mueller and Maeve McNamara. And it’s a picture of what goes wrong in the elderly compared to someone who can clear the infection. And what you’ll see is that there’s a cut through the lung. And what happens in the elderly is that the virus goes down into the lung, causes hyper immune response. And in the late stages of the disease in the elderly particularly, it’s a hyper immune response, which we call the cytokine storm. And what we’ve recently discovered, the planet that is not just my lab, is that the virus can attack the endothelial cells of the agent. And that’s not just in the lung, which of course is a problem for getting blood flow and oxygen across, but what’s also important is that these endothelial cells that line the blood vessels, particularly the micro capillaries, line at the heart, the brain, even the extremities.
And so what we’re seeing in elderly patients particularly that undergo this cytokine storm is what’s called a coagulopathy, which means that lining of the blood vessels is getting inflamed and causing clots to form. And you get a rise in this marker called the D-dimer, which is a breakdown product of clotting. And what we’re seeing is even in young people, there’s propensity for stroke, myocardial infarction, heart attack, and even things like numbing of the toes and the fingers. And you can see that there are what are called chilblains in some people, you get these dark areas on the body. So that’s particularly fatal if it’s not controlled and it’s very difficult to control that. So what’s behind all of this susceptibility to the agent?
Well, there are two things going on, mainly one is the inability to clear the virus initially. So if you’re young, you can have a spike in viral numbers. It starts to get in your throat, drift down into the lungs. But young people tend to not have this overreaction, they tend to form antibodies fairly rapidly and clear the viral. If you clear the virus very quickly, you’ll actually have very little risk of going into hospital or the ICU. As an aside, if you don’t have a very strong case of COVID-19, looks like you don’t mount a very strong immune response, but that’s another topic for a future discussion. What’s more important is to focus on: What is it about the aging immune system that’s defective that leads to their inability to clear the virus? And then the second part that’s important for the agent is: What happens once they start to clear the virus and why is that so detrimental?
And what we are seeing is that the virus particles, particularly the viral RNA, lasts a long time, sometimes for weeks in the body. And those remnants actually are what we think are stimulating this hyper-immune reaction cytokine storm, which is driven largely by a particular protein complex called the inflammasome, which is already hyperactive, chronically in the agent. And we’ll talk about that later on, but just to give a shout-out to my co-authors, their drawings were beautiful. So we’ll get back to the disease course in a moment. One of the things I want to bring up is one of the great things in this article that Amber and Maeve did was that they drew a table of respiratory viral infections and what are the risk factors? And so I have the table in front of me so I’ll just read off some of them, which you can see in the paper.
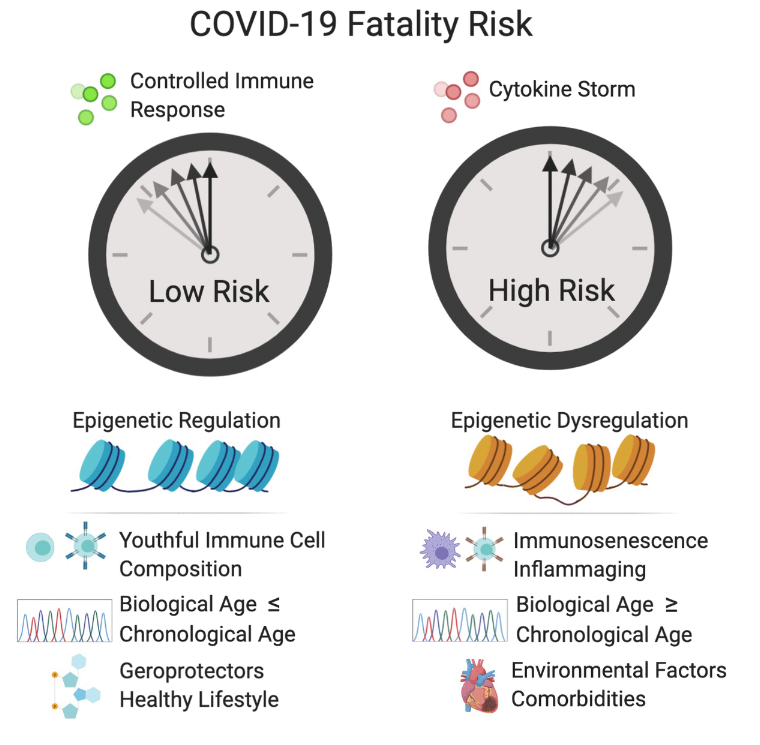
Mers in the original SARS, they actually had high risk. One of the risks was one in Type 2 diabetes, obesity, cardiovascular diseases, hypertension, old age, this is for Mers. For SARS one, it was again diabetes, renal disease, neurological diseases, metabolic, and interestingly dermatological diseases, which is probably an immune thing. But why is that important? What that tells us is that these particular type of corona viruses attack the agent, and in particular, the agent with underlying co-morbidities, these underlying diseases. But what I would like to us to consider and what I’d like to argue is that it’s not just about having obesity, having diabetes, having heart disease that is the problem. Those are symptoms of a more insidious problem, which is that those people are most likely older than their chronological age, or they’re actually very old biologically because they’ve lived a long time, but we know that biological age will be accelerated by being obese, by not exercising and just living the lifestyle that we know from epidemiology is not the perfect one.
At least half of America is overweight or obese. If you include certain cutoffs, some people estimate that it’s over 75% and this drives the aging process. And one of the side effects of course is obesity but obesity may not be the main driver actually, that’s a symptom of the problem that I want to talk to you about. So there are lots of things that go wrong in the aged body. And by age, I’m not just talking about birthday candles, I’m talking about actual biological age. Now biological age can be measured in a variety of ways. Let’s just talk about that for a minute. We can measure the DNA methylation status of ourselves, the so-called Horvath DNA methylation clock, we can measure that pretty easily in a blood test or a swab from the cheek these days get a very accurate estimation of how old someone is biologically.
But there are other things that change in a predictable way. And unlike 10 years ago where we thought we’d never have biomarkers, now we have quite a few. You can look at changes in immune cell diversity, such as T-cells, you can build a very good immune clock. You can look at the levels of NAD in the body, which decline with time. One of the things that we, Gordan Lauc and I, professor Gordan Lauc and I, wrote about is a paper actually also in the journal, Aging, is that the immune system changes in part because sugars change that are attached to proteins. This is the process of glycation and Gordan’s lab has done an amazing job, they’ve found that there’s a glycan clock and what he calls it is the glycogen age of a person.
And why is that important? Because as we get older, the type of sugars that are attached to proteins in the body, whether it’s antibodies or actually the coronavirus spike protein, and even the H2 so-called receptor on the surface of endothelial cells, these are all changed as we get older in terms of their glycation. And if you look at figure 3in the paper, you can see a beautiful rendition of these changes. And we also have epigenetic changes that control how cells behave. And we know that during aging, epigenetic changes occur, and we think that cells lose their identity. And that’s true for immune cells, it’s true for the lining of the blood vessels, the endothelial cells, and that may be why the virus has a greater chance of attacking an older person’s body as well.
And then finally, there’s the process of immunosenescence. Now that there’s two types of immunosenescence and I don’t want to get people confused here. Immunosenescence typically refers to just the aging of the overall immune system. That means that there’s less variety of T-cells. There’s less ability to mount an immune response and clear viruses, but there’s also cellular immunosenescence or what you call immuno. But there’s also cellular senescence which is a different story, which is about cells checking out of the cell cycle and becoming more like zombie cells. And you can stay in those for galactosidase or p16, and this is another type of cellular senescence.
There’s some overlap between the immunosenescence and cellular senescence, but it’s important to realize they’re not the same thing. And so that’s the lead-up to the whole paper, which goes into detail about these various causes susceptibility to viruses in general, but also to COVID-19. Now, one of the areas that we work on of course are the sirtuins. These are enzymes that our bodies make. There are seven of them in most of our cells, and they’re very important for fighting against diseases, both chronic diabetes, heart disease, Alzheimer’s, we believe based on a lot of mouse and human genetic studies. But also we’re finding are important for viral defenses. And we put forward a hypothesis in this paper that the sirtuin defenses are lost during COVID-19 infections. And one of the reasons for that is the following.
So sirtuins need NAD and unfortunately, as we get older, we think that a lot of our cells lose the ability to make an NAD effectively and they also destroy it for reasons that we don’t fully understand yet. But what we’ve also discovered in my lab and in others, Charlie Brenner put out a nice paper about this a few weeks ago, is that a virus, coronavirus and other types of viruses, deplete NAD in cells. And we think this is part of their defense, the viral attack and the inability of cells to survive the attack. Now they do this through activation of the PARPs. PARPs are poly ADP road to cell trans… polimeracion. So they do this by activating the PARPs, such as PARP1, PARP12, PARP14. And PARPs are enzymes that polymerize NAD and depleted from the cell. And we think that by either blocking the PARP activity or replacing, replenishing the NAD levels in infected cells and in the body of patients, we can give them a better chance of survival.
Now, why would we worry about NAD and sirtuins? Well sirtuins, particularly sirtuin 6, sirtuin 1, sirtuin 2, they control inflammation and they dampen it when it’s overactive. I mentioned the inflammasome. Well, one of the key components of the inflammasome is called NLRP3, and the acetylation chemical to that protein is what causes it to be active. Actually, if we deescalate of enzymes like CERT1, CERT2 deacetylate NLRP3, it brings that activity down. And so what we’re thinking is that when cells are infected, the NAD levels go down. So sirtuins are unable to dampen the inflammatory response and you get this cytokine storm. So in other words, if we were to raise NAD levels in patients, we may be able to prevent their bodies from going into this state of shock and aseptic like response.
Figure 2. Factors that increase the fatality risk of COVID-19.
Now I will admit, at first I didn’t think this was something that I should rush into. Of course, I would look like somebody with a hammer looking for a nail because you’d think that everything that I do looks like an NAD problem, but studies like the Brown paper that came out as well as studies over the last five years in my lab that have looked at NAD changes during macrophage activation and the PARP response have really pushed me into the belief that, as I write in this article with my coauthors, that NAD is part of this story. Now it’s not the whole story. In fact, the NAD story in this paper is only a small part of it, about 5%, but I want to talk about it because a lot of people are asking me, “David, what about NAD?” And interestingly, I’ve been working with a team in Boston on making an NAD precursor a drug.
And so for the last two years, with the help of a great team at Brigham and Women’s Hospital, they’ve been testing the safety and efficacy of an NAD precursor called MIB626, which is a proprietary version of NAD booster. So far, the molecule is extremely safe in the people that have been tested. It’s able to greatly raise NAD levels. Now there’s some debate out there in the Twitter-verse that the molecules that we work on in my lab and in these clinical trials don’t raise NAD and are not effective. Well, I can tell you that you probably shouldn’t get your scientific information from Twitter because it’s completely wrong. And now what’s interesting and exciting is that in the next few weeks, very extensive, double blind placebo controlled study is about to begin with this molecule. And we’ll see, pretty quickly I think, whether patients are helped by raising an NAD. Particularly the more severe ones.
Now, there are anecdotal case studies already. Some of them are online that you can look up if you’re interested, of patients recovering quite rapidly, supposedly, with treatment with NAD boosters like NMN, which is one of the ones that we work on. But those individual case studies don’t prove anything as we now know from having studied other molecules in other people’s study molecules in the world for COVID-19. So that’s why we’ve decided to do this very rigorous placebo controlled study and not just go for compassionate use. And we’ll see over the next few weeks, perhaps few months, realistically, whether this molecule that we’re working on is going to dampen the inflammatory response in patients that really need it. Drugs are very hard to make, most of them don’t work, so I’m not promising anything, I’m not expecting too much, but I think that we need to give this a shot.
And the other reason for believing in this work is that aging, as I started out in this review, in this talk mentioning, we think aging is the major driver of COVID-19 susceptibility. Aging of all of the different parts of the body in particular, the immune and circulatory systems. Now, if we can delay aging or reverse it, perhaps in some way with NAD boosting or with other drugs that are out there such as Metformin, which [inaudible] is arguing could be used to bring down blood sugar to improve the body’s survival. These kinds of longevity molecules could be used to bring not just the virus down, but boost the survival and the resilience and the defenses of the host up in the same way that you don’t just have weapons of war, you have the defenses as well.
And so on the defensive side, I think bringing up the defenses of the age is just as valid, if not more important than attacking the virus itself. So why would I say, “It’s just as important or more important?” Well consider that this is not the only virus that’s going to attack humanity going forward and vaccines while they’re great and we hold out full on. It probably won’t work against the next outbreak, whether it’s bird flu, regular flu, or another coronavirus, or even a mutated version of this one that’s out in the population. So we need to work also on the body’s ability to fight infections, in general.
So with that, I think I should let you all go. I’ve talked long enough about this paper. I hope you enjoy it. We really enjoyed writing it. It was challenging I’ll admit because it was written in real time as data was coming in and do a lot of things to update. And I’m grateful to Aging, the journal, for making papers available and published within rapid time. And I can tell you that the review process, the peer review process, was extensive. We’ve got pages and pages of comments from reviewers that really helped, particularly in this case. So, enjoy the paper and I’ll keep you updated through my other social media, but also through papers that we hope to publish in the next few months.
Thanks, take care.
Click here to read the full study published by Aging.
Aging is an open-access journal that publishes research papers monthly in all fields of aging research and other topics. These papers are available to read at no cost to readers on Aging-us.com. Open-access journals offer information that has the potential to benefit our societies from the inside out and may be shared with friends, neighbors, colleagues, and other researchers, far and wide.
Behind the Study is a series of transcribed videos from researchers elaborating on their recent oncology-focused studies published by Aging. A new Behind the Study is released each Monday. Visit the AgingYouTube channel for more insights from outstanding authors.
—
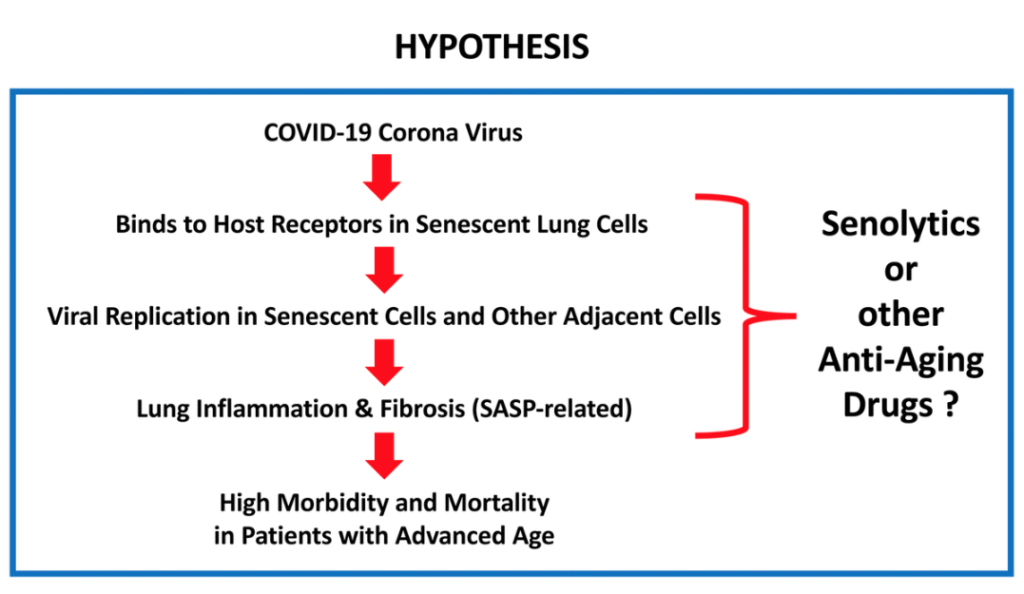
Hi, I’m professor Michael Lisanti and I’m the Chair of Translational Medicine at the University of Salford, and today I want to talk about our new prospective article, which links COVID-19 and chronological aging, and is focused on potential treatments and prevention strategies. I got interested in this topic because there seems to be an association between COVID-19 fatalities and aging, especially in patients with advanced chronological age. Patients over 65, and their 70s and 80s, are more likely to have increased morbidity and mortality. And so, I thought there may be a link there, between aging and senescence and the viral replication, as well as the potential therapy.
What I’d like to highlight about this particular article is that it proposes potential treatment strategies as well as prevention strategies. The reason is because it appears that this disease, the virus itself, may target senescent cells and senescent cells have been rewired to increase protein synthesis and also to increase the secretion of inflammatory mediators, which is known as the SASP, the senescence-associated secretory phenotype.
And so, one idea would be to use drugs that are senolytics. Senolytics are drugs that target and lyse senescent cells, but also to use protein synthesis inhibitors. The reason is because proteins synthesis inhibitors and senolytic drugs would prevent viral replication, which would reduce viral transmission. And so this could be used as a preventative strategy. I’ll just give you a couple of examples. If you have a drug which is an FDA-approved protein synthesis inhibitor, it should inhibit the secretion of inflammatory mediators, like IL-6. It should inhibit the fibrosis by preventing the secretion and production of collagen. And most importantly, the virus is also made of protein, so if you have a protein synthesis inhibitor, it will also inhibit viral replication.
Figure 1.What is the relationship between COVID-19 and advanced chronological age?
There are three drugs I’d like to mention in particular. One is azithromycin, which is a senolytic. The others are also protein synthesis inhibitors, like doxycycline and rapamycin. All three have been shown to reduce IL-6 production because of their inhibition of protein synthesis activity. And also, all three of them have been shown to inhibit viral replication, not specifically of COVID 19, but since this effect on protein synthesis is a generalized effect, it should work for any virus. For example, azithromycin has been shown to inhibit the replication of Zika virus and Ebola virus, doxycycline has been shown to inhibit the replication of dengue virus, and rapamycin, which is another protein synthesis inhibitor with anti-aging properties, has been shown to inhibit replication of the HIV virus.
So, it seems to me that it’s a no-brainer that we should be repurposing FDA-approved drugs that are protein synthesis inhibitors, both for prevention, to prevent the inflammation fibrosis that’s occurring that’s killing people with COVID-19, and also to prevent the contagion by inhibiting viral replication. So I think this could provide a very inexpensive way forward because drugs like doxycyclin are only less than 10 cents a day, and could be used, as I said, for both prophylaxis and treatment. But, I think we need to use it early in the disease to prevent the fibrosis and inflammation, which makes them long, very inflexible and unable to expand and contract, and leads them to a fibrotic lung disease, which prevents patient recovery and could explain lethality of the disease.
I would like to directly engage with people to pick this up, to bring this forward as potential clinical trials. These clinical trials could be done directly in healthcare workers because they are the most vulnerable. In addition, they could be done in patients with advanced chronological age, or even with patients that are asymptomatic, that have been identified as the virus-positive. And it would be like a window trial where you would do viral titers first, and then you would give the drug and then you could also look at the viral titers after administering the drugs. So this would be a very easy, straightforward trial.
All the diagnostic tools for COVID-19 have already been identified and perfected, so all we need to do is interject FDA-approved drugs, which are protein synthesis inhibitors, to look at the eradication, the virus. So this would also be a very inexpensive clinical trial. But I would like to engage with infectious disease experts and virologists to help facilitate. Thank you.
Of course, I would like to thank two foundations which have supported our work: The Fox Point Foundation in Canada and The Healthy Life Foundation in the UK for providing the equipment and infrastructure at the University of Salford.
Click here to read the full paper, published by Aging.
Aging is an open-access journal that publishes research papers monthly in all fields of aging research and other topics. These papers are available to read at no cost to readers on Aging-us.com. Open-access journals offer information that has the potential to benefit our societies from the inside out and may be shared with friends, neighbors, colleagues, and other researchers, far and wide.
Aging Editorial Board member Dr. Alex Zhavoronkov discusses his 2020 research paper published by Aging, entitled, “Geroprotective and senoremediative strategies to reduce the comorbidity, infection rates, severity, and lethality in gerophilic and gerolavic infections.”
Researchers explain their studies that were published in Aging
Behind the Study is a series of transcribed videos from researchers elaborating on their recent oncology-focused studies published in Aging. A new Behind the Study is released each Monday. Visit the AgingYouTube channel for more insights from outstanding authors.
—
Hello, my name is Alex Zhavoronkovand I’m the Founder and CEO of a company called Insilico Medicine. We are focused on the latest applications of artificial intelligence to drug discovery, biomarker development, and aging research. And I’m also a Chief Scientist at the Biogerontology Research Foundation. It’s a UK-based charity, 12 years old now founded in 2008. It’s called the Biogerontology Research Foundation because it’s focused primarily on biological and biomedical gerontology with support research worldwide. And we also conduct policy outreach, policy documents, and promote aging research worldwide.
We got into the coronavirus theme in mid-January as a company and also as an extended group of collaborators. At Insilico, we decided to go directly after viral proteins. So we have the ability at Insilico to identify new targets, but also to generate normal compounds very quickly using generative cell networks and reinforcement learning. So it’s kind of imaginative and strategy oriented AI to create molecules that specifically bind to the proteins of interest.
So we originally published and put out the paper and the molecules for the 3C-like main protease of the SARS-CoV-2. And we’re working with multiple collaborators worldwide to provide the molecules for their proteins of interest, and also we are generating a bunch of others. However, for the purposes of this paper we are not using AI in any way. It’s human intelligence and it is quite obvious that SARS-CoV-2 is more harmful to the elderly, the people over 50. So it’s infecting more people over 50, it is a much more severe and much more lethal in that age group.
So that is why it’s actually pretty unique compared to other viruses. So if you look at influenza and the other common viruses we do not see another virus, we do not see such effects in the elderly, so it’s a little bit more equal opportunity infections. For SARS-CoV-2 it infects mostly the elderly and there is actually no term to describe it right now. So in the paper that I put forward in Aging, I propose a new term so it’s gerophilic and gerolavic infection from Greek géros, old man and epivlavís, harmful. So it’s more harmful to the elderly, more severe in elderly. And gerophilic it’s géros again old man and philia is love, so it loves old people.
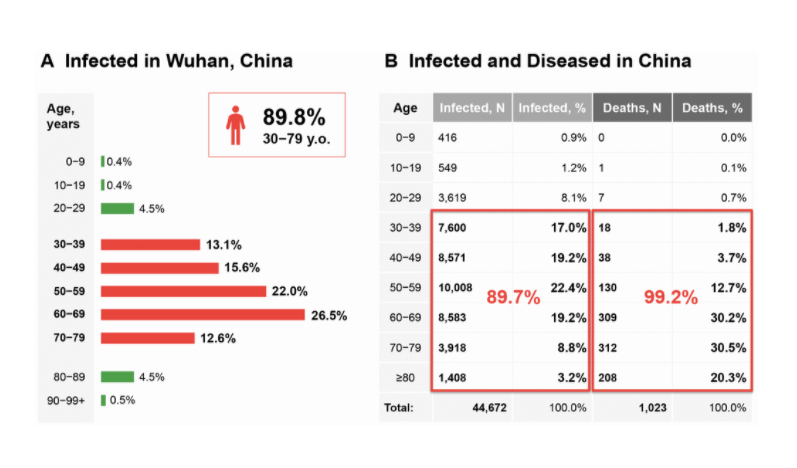
And if we’ll look at the data from Wuhan in China, you will see that 90% of the population, 89.7% of the population, who got the virus were over 30. And 99.2% of the population that died of it were over 30. So it’s really uneven distribution for both severe cases and lethal cases in the population. And one of the really important case studies that has been studied quite extensively is the Diamond Princess cruise ship. So the world’s most watched lab that came into attention because a few thousand people got stuck, very diverse population group was stuck on one cruise boat. And out of those few thousand, around 700 contracted the virus and most of them were over 65 and there were originally seven deaths, and a few more people died.
Figure 1.COVID-19 as a gerophilic and gerolavic infection.
And we see that people who had the infection, even with mild symptoms, they have dark spots in their lungs on CT. So it looks like they have some lesions and there is some fibrosis. Even if the disease has mild symptoms, in the elderly more so, it leaves the fibrotic trace. And in the paper, I’m hypothesizing that the disease is associated with immunosenescence. So both the involution of the thymus and many other processes that lead to immunosenescence. Immunosenescence leads to infection, so here you have of course chances of death. Infection leads to more damage and loss of homeostasis and that leads to accelerated aging. And also acceleration of age-related pathology also increase the chances of death that lead to more immunosenescence. So it’s kind of the vicious circle of immunosenescence and infection.
And there have been many studies in the past showing that some of the geroprotectors like sirolimus, rapamycin, are maybe effective in potentiating response to vaccines and also preventing infection in the elderly. So it’s paradoxical observation that immunosuppressant, like rapamycin, might have immunostimulatory effects. And there was anecdotal evidence showing that it protects the elderly from influenza and other virus not infections. It’s pretty obvious to try something like rapamycin that is reasonably safe in low doses. So in high doses it has substantial side effects, but in low doses it’s very well tolerated.
So there are others what is called rapalogs, very famous one is called everolimus. It’s so very close structural analog to sirolimus, developed by Novartis which has claimed to be selective to specific coattails and outdoor complex that make it more beneficial for aging and for other diseases. However, I would really like to see more evidence of that because those are very close structural analogs and there are other inhibitors that serve the same purpose. So 2013, Novartis conducted few experiments with everolimus, the drug is called RAD001 and demonstrated that in healthy elderly patients a low dose treatment with RAD001. Results in even potentiation and less infection with influenza and also potentiation of vaccines. So that was promising news.
So they published in 2014 in Science Translational Medicine and it was very promising study. Then in 2018, they showed that a combination of everolimus and another ToR inhibitor also results in immune potentiation and prevention of several infections, primarily influenza. So for influenza, they published in Science Translational Medicine, and a spinoff out of Novartis took those molecules into clinic, into Phase 3. And in Phase 3, they decided to instead of using everolimus, they used the molecule called BEZ235 rebranded as RTB101 which had high concentrations. It’s also a PI-3K inhibitor, so it’s not a very selective inhibitor or ToR, and they failed in Phase 3.
But they haven’t used RAD001 or sirolimus in combination or as control. I believe that it’s likely to be because of the molecule and also patient selection, so it should be biomarker used for that. But those promising early experiments clinical studies with RAD001 and also substantial evidence from the clinic met-studies showing that rapamycin is potentiating a vaccine response and immune status in the elderly. That gives us very promising data to try sirolimus in Phase 3 in low doses maybe once a week, maybe in combination with other geroprotectors like metformin, like NAD boosters, like senolytic to potentiate the immune system of the elderly before they get sick.
So in this paper, I also want to highlight that it’s not a medical advice, it’s not a recommendation, it’s a call for a clinical trials of an alternative view on how to address COVID-19 also SARS-CoV-2 and prevent infection and increase survival in the elderly, and also make it less severe for the elderly. So in this paper, I’m calling for clinical trials of rapamycin, a very well known geroprotector. It was actually implicated in Aging by Professor Mikhail Blagosklonny at Roswell Park in early 2000s. So 2004, 2005, 2006 with seminal papers showing that cancer agent is very likely to be also an anti-aging compound, and I now believe that this compound should be tried in multiple age associated pathologies and also for immmunosenescence, versing immunosenescence.
But other geroprotectors, promising geroprotectors, like metformin, can be very well combined with rapamycin, NAD boosters like nicotinamide riboside, nicotinamide mononucleotide may be tried in clinical trials. Senolytic, these could be tried also after COVID because of the fibrotic build-up, fibrosis in the lungs and also as rehabilitation after COVID. I think that some other promising geroprotectors including [inaudible] B3 activation. Again, that’s much less explored, could lead to gene clocks. So since 2013 there has been a revolution in gene clocks starting from our Panam and Horvath work showing that methylation data is very predictive of chronological age.
There are very highly accurate markers of aging but there are many others, so like lab tests, very simple clinical blood tests can be used to predict chronological age and my group published the first ones using deep learning. And there are many others including microbiomics aging clock, including imaging aging clocks, including transcriptomic aging clocks, and proteomics aging clocks, and whatever data there is longitudinal data that could be used to construct clocks should be collected during the clinical trials. And we should look at whether some of the molecules are making you younger or older compared to the chronological age from the various data types and look at the effects.
So that’s the current proposal on the paper, so I’m calling to try geroprotectors to protect the elderly, to potentiate their immune response to COVID, and also to try the aging clocks for both clinical trials enrollment and for monitoring to see what molecules are making you younger or older on pretty much every level. I’m also calling for those clinical trials because after COVID-19, after the epidemic is over, we’re going to have major economic consequences. There’s a lot of people who have been out of work, there’s been substantial capital influx from pretty much every government into the economy, so quantitative easing that might lead to inflation. We don’t know what’s going to happen to the economies of developed countries.
Previously, I published several papers and a book on economics of aging showing that increases in productive longevity would lead to substantial economic growth. If we manage to reduce the amount of money being spent on healthcare in the elderly by preventing disease and by rejuvenating the elderly, making them more resilient to disease, just that leads to unprecedented economic growth. And of course, if we make them more productive and contributing to the labor force longer, we will see unprecedented economic growth even further.
So we’re talking about double digit growth in developed countries. So here we can kill many birds with one stone, so to speak, even though I don’t like the word “kill.” And if we can try geroprotectors to prevent disease, but at the same time we can boost the economy after the epidemic is over if some of those geroprotectors show efficacy and people start believing more that aging is plastic and we can push the envelope in that area and really rejuvenate the elderly.
So that’s the paper and thank you very much for watching this. Stay healthy.
Click here to read the full study published in Aging.
—
Aging is an open-access journal that publishes research papers monthly in all fields of aging research and other topics. These papers are available to read at no cost to readers on Aging-us.com. Open-access journals offer information that has the potential to benefit our societies from the inside out and may be shared with friends, neighbors, colleagues, and other researchers, far and wide.